Bariatric programs in the United States carry a structural mismatch between intake demand and surgical capacity. Patients now arrive earlier in the funnel and often after a year on a GLP-1 medication that did not reach their goal, expecting a clinical pathway that already knows their numbers. The verification stack most programs still rely on — a self-reported weight, an in-clinic tape measurement, a manual BMI computed during the consult — was built for a slower era of demand.
This guide is for bariatric clinic administrators, program directors, and pre-authorization coordinators who own that intake stack. It covers why pre-qualification is the gateway to hardening first, how mobile body scanning fits into the pre-consult and pre-auth workflows, and where structured remote body data delivers operational value.
Disclaimer. Mobile body scanning solutions described in this article do not determine medical eligibility for bariatric surgery, provide diagnoses, replace clinical evaluations, or make pre-authorization decisions. They produce body measurement and composition data intended as supporting evidence within decisioning workflows operated by licensed bariatric programs and their compliance and payer counterparts.
Why bariatric programs need faster pre-qualification
The demand-side numbers have been moving in the same direction for years. The CDC’s most recent NHANES data show 40.3% of US adults have obesity and 9.4% have severe obesity, measured by BMI ≥30 and ≥40, respectively, across the August 2021–August 2023 cycle. That puts the clinically eligible population in the tens of millions — an estimated 33 million US adults meet eligibility criteria, yet fewer than 1% complete surgery in any given year.
The supply side has stayed roughly flat. The American Society for Metabolic and Bariatric Surgery (ASMBS) estimates that 270,089 metabolic and bariatric procedures were performed in the United States in 2023, down roughly 3.5% from the prior year, with sleeve gastrectomy accounting for 58% of the total.
The gap between eligibility and completion is an operational problem. Bariatric programs run on a finite number of consult slots, OR days, and pre-authorization coordinators. When intake demand rises while surgical capacity remains unchanged, the bottleneck shifts upstream into the verification and documentation steps that determine whether each consult slot becomes a procedure or a deferral. That is the section of the workflow most exposed to inefficiency, and it is where a remote scan-derived body-data layer is built to help.
The intake gap: when eligibility gets confirmed too late
The standard bariatric intake still leaves a meaningful share of clinical verification to the in-person visit. The patient self-reports a starting weight on an online form, the program books the initial consult, and the body measurement step occurs at the appointment. Eligibility is confirmed at the visit rather than beforehand, and the consult slot becomes a measurement-collection event as much as a clinical conversation.
Two problems sit underneath that design. The first is data quality at intake: CDC researchers reported in Preventing Chronic Disease that self-reported BMI underestimated the prevalence of severe obesity by 40% — 5.3% on self-report versus 8.8% after bias correction in 2020 data. For a program where BMI is the eligibility trigger for several procedure types, a self-reported value serves as a placeholder that must still be verified in person.
The second problem is attrition: pre-operative dropout rates of up to 50–60% are reported across bariatric programs, with patients leaving at every stage between the initial consult and the surgical date. Each lost patient represents consult-slot, evaluation, and pre-auth coordinator time that the program has already spent. When the eligibility signal at the top of the funnel is noisy, more of that downstream effort gets spent on patients who will not reach surgery.
Consult schedules fill quickly, but the conversion from consult to procedure does not move in proportion, and pre-authorization documentation cannot begin in earnest until measurements have been collected in the clinic. The verification step is happening at the wrong place in the pathway.

Discover how AI-powered body intelligence is reshaping GLP-1 programs, telehealth, and digital health, from accurate remote assessments to safer and more engaging patient journeys.
The GLP-1 shift: volume contracted, intake complexity rose
The first instinct in 2024 was that GLP-1 medications would replace bariatric surgery. The 2025 intake picture turned out more nuanced. GLP-1 medications have not replaced bariatric surgery — they have changed who arrives at the consult and when. Procedure volume contracted in 2023, while bariatric program leaders report rising new-consult volume from patients who started on a GLP-1 and escalated. For programs, this means more upstream intake to triage with the same surgical capacity downstream — making faster, structured pre-qualification more valuable, not less.
The volume contraction is documented. An analysis of 17 million privately insured US adults with obesity in JAMA Network Open found that bariatric surgery use fell 8.7% between 2022 and 2023, while GLP-1 prescribing in the same cohort more than doubled. The ASMBS 2023 estimate cited earlier shows the same direction in the broader population.
The rise in intake complexity is documented within the program director community. In an American College of Surgeons Bulletin analysis published in April 2025, Luke Funk, MD, MPH, FACS, a bariatric surgeon at the University of Wisconsin-Madison, described GLP-1 medications as “the initial gateway for a lot of patients” who later move toward surgery. Marina S. Kurian, MD, FACS, clinical professor of surgery at NYU Langone Health, reports in the same article, “Most of my colleagues around the country are seeing an increase in new consults coming for surgery,” as anti-obesity medication use rises.
The coverage backdrop is consistent with that pattern. KFF’s 2025 Employer Health Benefits Survey reported that 43% of firms with 5,000 or more workers covered GLP-1 agonists for weight loss in 2025, up from 28% the prior year. That route is pulling more patients into the weight-loss care pathway, and some of them eventually reach a bariatric consult.
The net effect is a wider, more heterogeneous intake funnel feeding the same surgical capacity. The patient at the top of the funnel arrives with a longer treatment history and tighter expectations about how quickly the program can confirm eligibility — so the intake step now carries more weight than it did three years ago.
What FitXpress captures, and how
FitXpress by 3DLOOK is a mobile body-scanning solution built around a two-photo guided flow. The patient takes a front and side smartphone image through a capture sequence that runs in roughly 45 seconds and requires no specialized hardware, producing 80+ body measurements, BMI, weight estimation, and body composition outputs.
Three properties matter for the bariatric use case:
- Time-stamped, structured outputs. Each scan generates a record containing the capture timestamp, validation outcomes, and the underlying measurement set, in a machine-readable format — the building block of an audit-ready intake and documentation trail.
- Remote capture. The scan is completed outside the clinic on a standard smartphone, removing the appointment slot as the verification gate.
- Compliance posture. FitXpress is HIPAA-maintained for US healthcare contexts and supports Business Associate Agreement (BAA) execution, with photos moving over TLS and stored on AWS S3 with SSE-S3 server-side encryption. Personal identifiers are not processed, and captured images are deleted immediately after processing or within a configurable retention window, depending on program policy.
The same underlying technology is described in more depth on the 3DLOOK technology page, and it is the foundation behind FitXpress’s telehealth and weight-loss deployments outside the bariatric context.
Pre-qualification: structured body data before the consult

Pre-qualification is the use case where the consult-to-procedure conversion math changes fastest.
Use Case Summary: Bariatric Pre-Qualification
- Industry: Bariatric clinics, surgical weight-loss programs
- Problem: Eligibility confirmed too late in intake; consult slots spent on measurement collection rather than clinical evaluation
- Solution: FitXpress remote two-photo scan delivers structured body data before the appointment
- Outputs: BMI, 80+ body measurements, body composition estimates, time-stamped audit trail
- Role: Pre-consult intake step — supporting evidence for clinical review, not clinical decision-making
- Business value: Higher consult-to-procedure conversion; reduced measurement-only visits; earlier documentation start
The pre-qualification workflow has four stages, and the redesign moves the body-measurement step from stage three back to stage one.
- Stage 1 — Remote scan at intake. After the patient submits a baseline questionnaire on the program’s intake form, the program sends a FitXpress scan link, and the patient completes the two-photo guided capture on their own smartphone (typically the same day). The scan returns the program a structured record containing BMI, 80+ body measurements, and body composition estimates.
- Stage 2 — Pre-consult review. A program coordinator or clinical reviewer checks the scan output against the program’s eligibility thresholds — procedure-specific BMI ranges, body composition signals, and any program-specific intake criteria — before scheduling the consult. Patients who clearly meet criteria move into a clinical-evaluation consult; patients who fall outside criteria are routed into the appropriate medical-management or referral pathway without occupying a surgical consult slot. The program’s BMI verification capability provides the underlying signal here.
- Stage 3 — Clinical consult. The visit opens with the scan data already in the patient’s record, so the clinical conversation can move directly to history, comorbidities, surgical risk, and patient education rather than starting with manual measurement. The consult slot becomes a clinical evaluation rather than a measurement-collection event.
- Stage 4 — Documentation handoff. The same scan record that supported the eligibility decision is available to the pre-authorization coordinator from the start of the case, rather than being assembled after the consult.
The mechanism here is not clinical decision-making. The scan does not determine whether a patient is medically eligible for surgery — the bariatric program makes that decision. What the scan supplies is a structured, verifiable body-data signal the program uses to triage which consult slots are opened, in what order, and with what supporting record already attached.
Pre-auth documentation: cleaner packets, fewer delays

Pre-authorization is where bariatric program operations meet payer operations, and where intake decisions either accelerate or delay the path to the procedure.
A standard bariatric pre-auth packet typically includes documented BMI history, confirmation of comorbidities, prior weight-loss attempts, supervised diet program participation, when required, psychological evaluation outcomes, and a body-measurement record. Payer review windows commonly run from a few weeks to several months, depending on the payer, the procedure, the completeness of the initial submission, and plan-specific medical-necessity criteria.
Manual measurements taken at the consult and captured on paper or in a free-text note are difficult to audit at this stage. A reviewer at the payer cannot independently verify the capture conditions, the time of measurement, or whether the measurement is consistent with other body-data points in the file. When the payer requests additional information — a documented BMI at a specific point in time, a body-composition signal, or a measurement record with a verifiable timestamp — the program has to either rely on a clinical note or schedule another in-person visit.
FitXpress changes the shape of that record. The scan produces a structured body-data file with a capture timestamp, validation outcomes from the guided capture, and the underlying measurement set in a machine-readable format. The program attaches that record to the pre-auth packet as supporting evidence, and the data is consistent across patients because the capture sequence is the same each time. Follow-up scans for serial documentation — a baseline at intake, a second capture before submission, a third before procedure — produce comparable records on the same timeline.
The anti-manipulation layer in FitXpress reinforces the audit posture. Live in-session capture (not a camera-roll upload), real-time pose validation, and built-in clothing detection address the manipulation patterns that payers and program compliance teams have started to flag in remote workflows. The underlying BMI verification architecture is the same one used in regulated weight-loss prescribing contexts.
The compliance posture matters at procurement. FitXpress is HIPAA-maintained, BAA-ready, and runs on encrypted-in-transit, encrypted-at-rest storage with role-based access controls. Photos are deleted immediately after processing or within a configurable retention window, depending on program policy. These are the floor a bariatric program needs from any vendor handling patient body data, and should be confirmed before any pilot begins.
Post-procedure: turning the baseline into longitudinal tracking
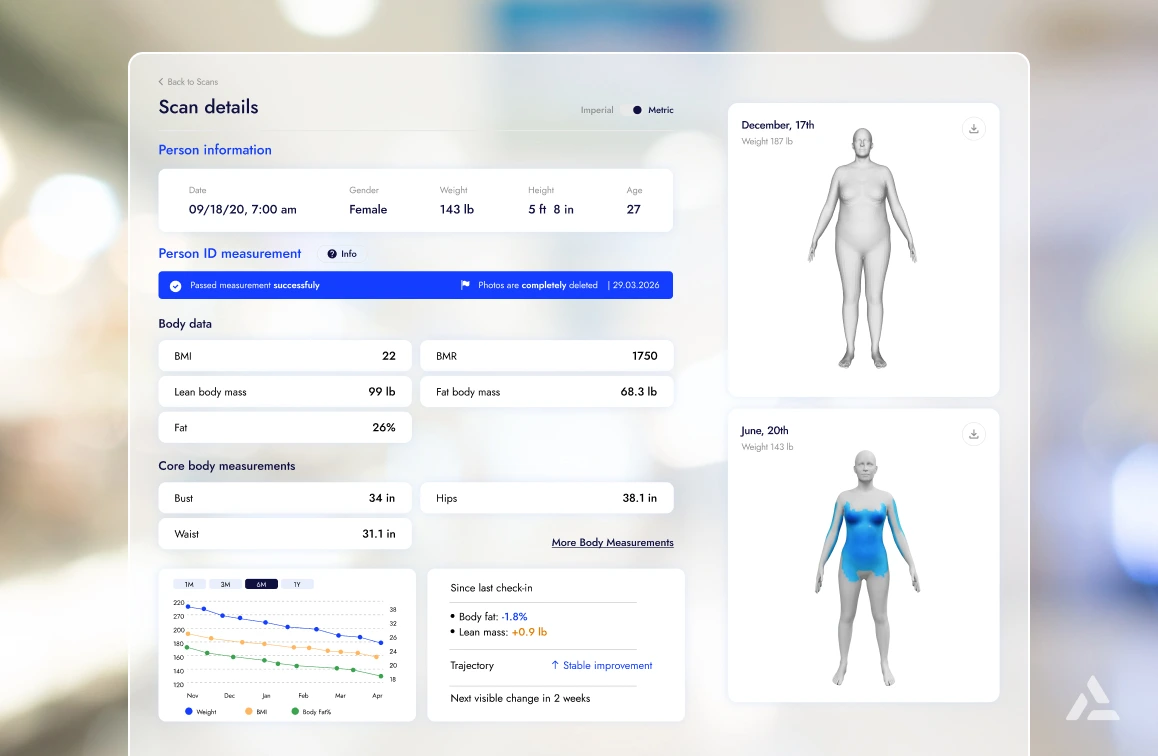
The first scan captured before surgery serves as a baseline against which follow-up scans are compared. The capture sequence is the same each time, so a scan taken three months after the procedure is structurally comparable to the baseline rather than a separate ad-hoc measurement.
The clinical value sits in the body-composition signal as much as in the measurement set. Weight alone does not describe a post-bariatric trajectory — the same weight can sit atop different body-composition profiles, and the difference matters for patient counseling, program-level outcome reporting, and the multidisciplinary care team (nutrition, behavioral health, surgical follow-up) supporting the patient after the procedure.
The adjunct-medication picture strengthens the case for longitudinal tracking. As the Johns Hopkins JAMA Surgery analysis found, roughly one in seven bariatric patients now initiate GLP-1 therapy after surgery — meaning the post-procedure phase increasingly includes a pharmacotherapy component alongside surgical recovery. A baseline scan, plus serial follow-up scans, provides the program with a body-data signal that is independent of medication adherence and is visible across the full post-procedure window.
A side-by-side body-data comparison between the baseline capture and a recent scan is also a tangible artifact for patient counseling, often more useful than a single weight number. The capture remains supporting evidence inside the program’s monitoring workflow, not a clinical decisioning output.
Where FitXpress fits in the bariatric patient journey
Across the full bariatric pathway, a single body-data capture asset supports multiple workflows. The structure below maps where each FitXpress capture event delivers value.
| Stage | FitXpress role |
| Inquiry | Remote scan captures early body data outside the clinic |
| Pre-consult | Supports pre-qualification review and consult-slot triage |
| Pre-auth | Provides structured, time-stamped documentation inputs |
| Procedure preparation | Establishes a baseline body-data record |
| Post-surgery follow-up | Tracks body measurement and composition changes over time |
| Long-term monitoring | Supports remote progress review without requiring a clinic visit |
One capture asset, applied repeatedly across the pathway, replaces a series of fragmented manual measurements and verification steps that today live in separate parts of the program’s workflow.
Why mobile body scanning beats manual measurement workflows
The differentiation is operational, not technological.
- No appointment slot required. Manual measurement workflows require an appointment slot, and mobile body scanning does not. The capture occurs on the patient’s smartphone, before, during, or after a clinical event, as the program’s workflow is designed.
- Cross-clinic comparability. Tape measurements vary by operator. A measurement taken by a medical assistant in clinic A is not directly comparable to one taken by a different medical assistant in clinic B, and neither is directly comparable to a self-reported measurement in the patient’s online intake form. Scan-derived measurements are machine-readable, produced through the same capture and processing sequence each time, and structurally comparable across patients and across time.
- Audit-ready records. Free-text measurement notes in the EHR are difficult to audit. A clinical note confirming a measurement was taken does not, on its own, allow a payer or compliance reviewer to verify the conditions of capture. In contrast, a scan record with a capture timestamp, validation outcomes, and a structured body-data file provides that audit posture by default.
- One asset, multiple workflows. The same capture supports pre-qualification at intake, pre-auth packet documentation, and post-procedure tracking. One capture asset, multiple downstream uses — that is what a bariatric program adopts, not a standalone imaging product.
The pre-operative attrition pattern noted earlier — up to 50–60% across bariatric programs — is why this matters. Every verification step that requires an in-person appointment is a point at which the patient can fall out of the funnel. Moving the body-measurement step upstream reduces that friction without touching the clinical decision rights that sit at the consult.
FAQ
Pre-qualification and pre-authorization
A program sends a remote body-scan link as part of the intake process. The patient completes the scan on their own smartphone, and the program receives structured body data — BMI, measurements, body composition estimates — before the consult. The data support pre-consult triage but do not replace clinical evaluation.
Bariatric pre-qualification is the intake step in which a program assesses whether a patient meets eligibility criteria — typically BMI thresholds, comorbidity profile, and program- or payer-specific intake requirements — before scheduling a full clinical consult. It is not a clinical decision; surgical eligibility determination remains with the licensed bariatric program after evaluation.
A structured body-measurement record with a verifiable capture timestamp can be attached to a pre-authorization packet, along with BMI history, comorbidity confirmation, and the standard clinical inputs payers require. The record helps payer reviewers verify capture conditions without relying on free-text clinical notes.
Moving body-measurement capture upstream — into a remote scan completed before the appointment — keeps consult slots focused on clinical evaluation rather than measurement collection. Patients who fall outside program eligibility criteria can be routed to medical management or referral pathways without occupying a surgical consult slot.
Mobile body scanning produces structured, time-stamped body data outside the clinic on the patient’s own smartphone. That single capture can support pre-consult review, pre-authorization documentation, and post-procedure tracking, eliminating the need for a separate measurement at each stage.
FitXpress generates structured body-data records — BMI, 80+ measurements, body composition estimates, and validation outcomes from the guided capture — that programs can attach to pre-authorization packets as supporting evidence within payer-side review.
No. FitXpress produces supporting body-data evidence for intake, documentation, and post-procedure monitoring workflows. Final clinical evaluation, eligibility determination, and surgical decision rights remain with the licensed program.
FitXpress provides a structured body-data signal before the clinical consult, so programs can identify which inquiries clearly meet eligibility thresholds and route the rest into appropriate medical-management or referral pathways. The screening signal is supporting evidence, not a clinical decision.
Post-procedure progress tracking
Patients can complete serial body scans at predictable intervals on their own smartphone, with each scan structurally comparable to the baseline scan captured before surgery. The program reviews longitudinal trends in BMI, body measurements, and body composition estimates as part of follow-up care.
The same weight number can sit on top of different body-composition profiles, so weight by itself does not describe the post-bariatric trajectory. Tracking body composition alongside weight provides the clinical team with a clearer view of changes in lean and fat mass.
BMI, waist and hip circumference, body composition (fat mass and lean mass estimates), and overall measurement trends are the most commonly tracked signals across bariatric follow-up programs. The specific set used depends on the program’s monitoring protocol and the post-procedure care plan.
Body composition tracking helps the clinical team distinguish lean-mass changes from fat-mass changes — a distinction relevant for nutrition, behavioral health, and surgical follow-up decisions that a weight number alone cannot inform. The tracking is supporting evidence within the program’s monitoring workflow.
A side-by-side body-data comparison between the baseline capture and a recent scan is a tangible artifact for patient counseling, often more useful than a single weight number on a clinic chart. Visual progress tracking can support engagement during the long post-procedure window.
A baseline scan captured before surgery, followed by serial scans at predictable intervals on the patient’s own smartphone, gives the program a body-data signal independent of medication adherence and visible across the full post-procedure window — the data support remote follow-up workflows without requiring a clinic visit.
About bariatric surgery
Bariatric surgery is a category of surgical procedures that alter the digestive system to support sustained weight loss in patients with severe obesity and related health conditions. Common procedures include sleeve gastrectomy, gastric bypass, and biliopancreatic diversion with duodenal switch.
Sleeve gastrectomy and Roux-en-Y gastric bypass are the two most common procedures performed in the United States, with sleeve gastrectomy accounting for more than half of the annual volume. Other procedures include biliopancreatic diversion with duodenal switch (BPD-DS), single-anastomosis duodeno-ileal bypass with sleeve (SADI), and endoscopic sleeve gastroplasty (ESG).
Programs evaluate a combination of BMI thresholds, comorbidity profile, prior weight-loss attempts, psychological readiness, and payer-specific medical-necessity criteria. Pre-qualification typically requires documented body measurements and BMI history.
Bariatric surgery is associated with sustained weight loss and improvement in obesity-related conditions such as type 2 diabetes, hypertension, and obstructive sleep apnea. Clinical outcomes vary by procedure type and patient profile.
Possible side effects include nutritional deficiencies, dumping syndrome, gallstones, surgical complications, and the need for revisional surgery in some cases. The program reviews these with each patient as part of the informed-consent process.
The clinical literature describes weight-loss surgery as the most durable intervention for severe obesity, with associated surgical risks, lifestyle adjustments, and follow-up requirements. The trade-off is patient-specific.
See FitXpress inside a bariatric intake
See how FitXpress can support pre-qualification, pre-auth documentation, and post-procedure tracking in your bariatric program. Request a FitXpress demo or contact sales@3dlook.ai.
Related reading
- AI in Insurance Underwriting: Mobile 3D Body Scanning for Remote Evidence Collection
- Wellness Rewards Verification for Employers & Insurers Using AI 3D Body Scanning