Use Case Summary
| Industry | Sponsors, Contract Research Organizations (CRO), academic research networks, and decentralized clinical trial (DCT) platforms running obesity and metabolic studies |
| Problem | Manual anthropometric measurement creates site-to-site variability, coordinator workload, and measurement-only visit burden in multi-site and hybrid obesity trials |
| Solution | Guided scan-based body measurement capture from two smartphone photos, deployable across sites and remote check-ins |
| Outputs | Structured, time-stamped body measurements, BMI outputs, and body composition estimates supporting protocol-defined measurement workflows |
| Role | Operational standardization and documentation layer for protocol-defined anthropometric measurement workflows |
| Business value | Reduced site-to-site variability, lower coordinator burden, fewer measurement-only visits, structured records that support monitoring and audit readiness |
Obesity and metabolic trials run on repeated anthropometric measurements. BMI, waist circumference, hip circumference, and body composition indicators can be captured at baseline, during follow-up visits, and throughout the post-treatment monitoring period. In a multi-site or hybrid trial, these measurements must be consistent — across sites, across staff, and across time points — for the data to support reliable longitudinal comparisons and protocol-defined endpoints. The harder operational problem is rarely the measurement itself; it is the measurement workflow. For teams evaluating clinical trial anthropometric measurement software, FitXpress provides a structured approach to capturing body measurements, BMI outputs, and body composition estimates across protocol-approved trial workflows.
This article is for clinical operations, CROs, pharma sponsors, academic research networks, and DCT platform teams evaluating how to standardize the capture of anthropometric measurements across obesity and metabolic studies. It covers how manual measurement workflows create variability and burden, how scan-based capture can support standardization across sites and remote check-ins, and the compliance scope FitXpress is — and is not — designed for in a clinical trial setting.
FitXpress use case in one sentence: FitXpress helps sponsors, CROs, academic research networks, and decentralized clinical trial platforms standardize the capture of scan-based anthropometric measurements across site-based, hybrid, and remote obesity trial workflows.
Scope note. FitXpress is a tool for operational standardization and documentation for clinical trial workflows. It does not replace protocol-defined reference methods, such as DEXA or circumference measurements performed by trained anthropometrists, nor does it independently validate clinical endpoints. The full clinical and regulatory scope is set out later in this article.
Manual measurements create avoidable variability in obesity and metabolic trials
Obesity and metabolic trials commonly rely on repeated anthropometric measurements such as weight, BMI, waist circumference, hip circumference, and body composition estimates or related indicators. Obesity-related studies registered on ClinicalTrials.gov frequently use these measurements as primary or secondary outcomes, measured at protocol-defined time points across the study window.
In a multi-site trial, the manual measurement workflow varies by site, staff member, tool used, technique, participant preparation, and documentation habit. Even when the protocol specifies the measurement method — anatomical landmarks, tape positioning, posture, equipment — real-world execution can introduce inconsistencies that the protocol cannot fully control. A trained coordinator at one site may measure waist circumference slightly differently from a trained coordinator at another site. A participant measured first thing in the morning may produce different numbers than one measured at the end of a long day of visits. Documentation conventions can drift over the course of a twelve-month study.
For sponsors and CROs, that variability is an operational risk before it is a data risk. It increases site burden, complicates monitoring, makes case review harder, and creates friction for participants — particularly when a visit exists primarily to capture body measurements that could, in principle, be collected outside the clinic. Much of this variability stems from the practical capture workflow around the measurement: who performs it, how the participant is prepared, how the measurement is recorded, and how consistently the process is repeated across visits.
What causes measurement variability in multi-site obesity trials?
Manual anthropometric measurements can vary across sites because of differences in staff technique, tools, training, documentation practices, and protocol execution. Even with a clear protocol, real-world capture is sensitive to local workflow decisions that accumulate over time and across sites.
Hybrid and decentralized trials need consistent remote measurement workflows
Hybrid and decentralized trial models continue to expand. Sponsors and CROs are utilizing remote check-ins, decentralized visits, and patient-centric workflows to improve recruitment, retention, access, and participant convenience — particularly in obesity and metabolic studies, where the study window can last 12 months or longer and where in-person, measurement-only visits add significant burden.
The trade-off is structural. Remote workflows reduce the friction of a clinical visit, but they only work for measurement data if the capture remains structured, repeatable, and reviewable. Anthropometric measurements are particularly sensitive: small differences in process, posture, or capture context can affect longitudinal comparability across visits and across the study population. A hybrid trial that relies on inconsistent remote measurement data may create more monitoring overhead than the in-person workflow it replaced.
This is where scan-based, time-stamped capture fits. It moves the measurement step into a guided digital workflow that can be deployed both at sites and during remote check-ins where the protocol allows, and it produces structured outputs that are easier to compare across time points. The goal is not to remove the site from the trial — it is to remove the measurement-only friction around the site visits without losing capture consistency.
How can decentralized trials collect body measurements remotely?
Decentralized trials can collect body measurements remotely via structured digital workflows that guide participants or coordinators through standardized data capture, generate time-stamped records, and produce outputs that support monitoring and review. The protocol determines which measurements can be captured remotely and at specific timepoints.
FitXpress: scan-based body measurement capture for obesity and metabolic trials
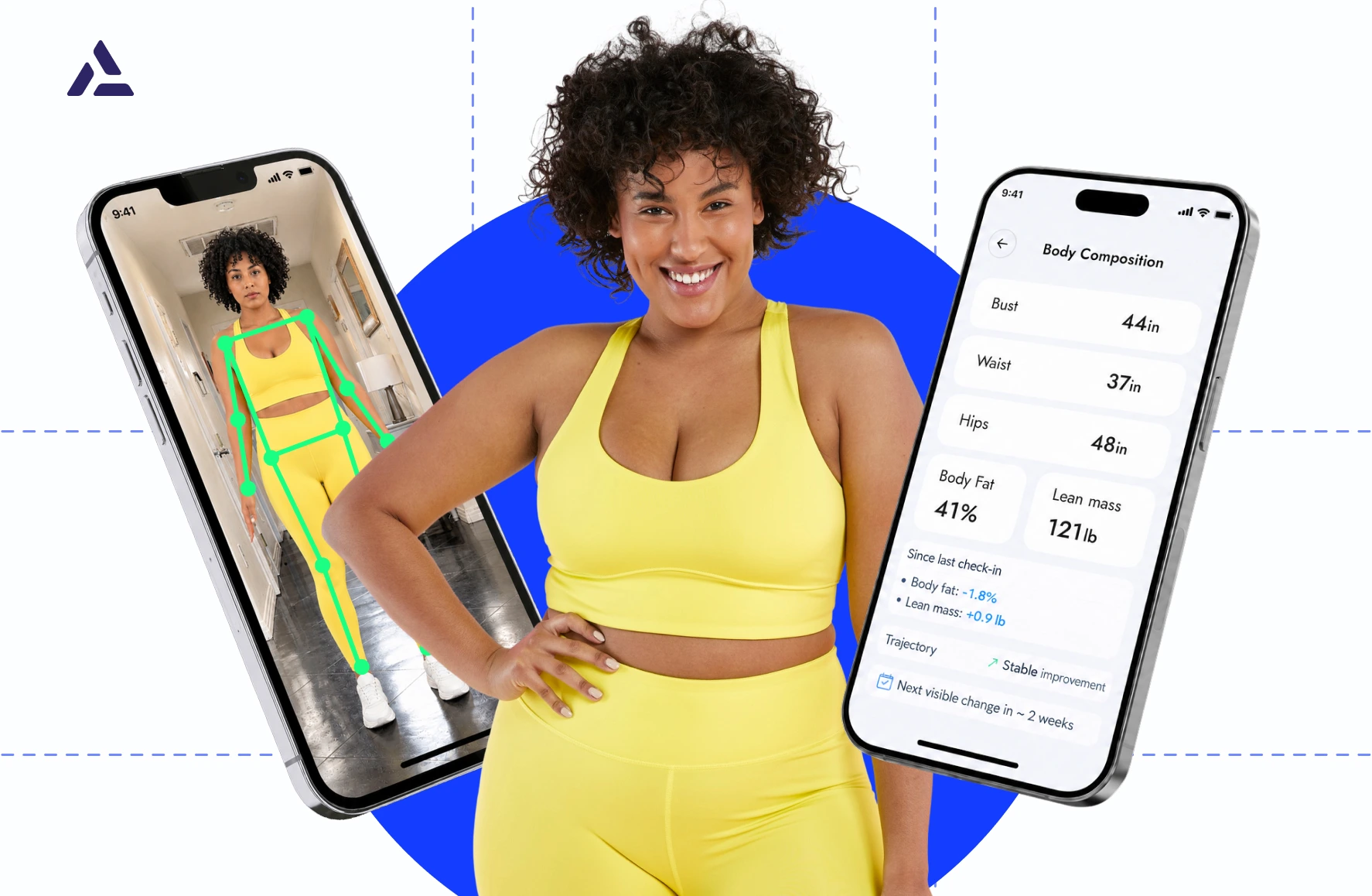
FitXpress is a mobile body-scanning solution built around a guided two-photo workflow. The user — either a participant or a coordinator assisting with capture — takes front and side smartphone photos and provides required inputs such as height, weight, age, and biological sex. FitXpress returns a 3D body model and structured body data, including over 80 body measurements, BMI outputs, and body composition estimates, with results processed in roughly 45 seconds. No specialized hardware is required.
The underlying technology stack is described in more detail in the section on how 3DLOOK turns two photos into structured body data. For the clinical trial context, three properties matter:
- Standardized guided capture. The capture flow remains the same across users, sites, and time points. The participant or coordinator follows the same guided sequence each time, reducing the process variability introduced by manual workflows.
- Structured, time-stamped outputs. Each scan generates a machine-readable record that includes a capture timestamp and capture-quality checks from the guided flow. The same data structure is used for baseline, follow-up, and remote check-ins.
- Deployable across site-based and remote workflows. The scan can be completed on a standard smartphone, allowing it to run during a coordinator-led site visit or a remote check-in as permitted by the protocol.
FitXpress is positioned as an operational standardization and documentation layer for clinical trial workflows — a means to capture anthropometric data consistently across sites and time points. It is not a replacement for protocol-defined reference methods such as DEXA, certified manual anthropometry, or other validated measurement protocols, and it does not independently validate clinical endpoints. Endpoint definition and validation remain protocol-level decisions made by the sponsor and the investigator team.
How FitXpress supports site-based, hybrid, and remote measurement workflows
The same capture workflow can run inside three trial-operations contexts: site-based visits, remote check-ins between visits, and remote pre-checks before a participant arrives at the site. The protocol design determines which of these are permitted for a given study and a given measurement time point.
Site-based baseline and follow-up visits
A coordinator uses FitXpress to capture standardized body measurements during a scheduled site visit. The workflow can replace or supplement protocol-permitted manual measurement steps where scan-based capture is permitted within the study design — such as tape positioning, recording into the site’s documentation system, and manual review — with a guided scan that produces structured output directly. The coordinator continues to handle protocol-defined steps that fall outside the scan, and the scan adds a consistent body-data record alongside those steps.
The operational gain is a repeatable structure. Site-to-site comparison becomes easier because the capture sequence is the same at both sites A and B, and longitudinal comparison becomes easier because the baseline scan and the month-twelve follow-up scan produce the same data structure.
Remote check-ins
Where the protocol allows asynchronous measurement-only check-ins, the participant can complete the same guided scan on their own smartphone at home. The capture produces the same structured output as the site-based scan, so a hybrid trial design can interleave site visits and remote check-ins without compromising data continuity.
Remote check-ins are best suited to two scenarios: capturing between-visit progress during the active phase of an obesity or GLP-1 study, and post-treatment monitoring during the extended follow-up window. In both, the alternative is either a measurement-only site visit (which adds participant burden) or no measurement at that time point (which creates gaps in the longitudinal record).
Remote pre-checks and eligibility support
In some study designs, the protocol allows for a remote body-measurement pre-check before a participant arrives at the site. The pre-check can surface eligibility-relevant data earlier in the workflow — for example, BMI-based screening criteria — and may help reduce avoidable screen failures by identifying participants who fall outside the protocol’s measurement criteria before the site visit.
The compliance scope on pre-checks is narrow. FitXpress supports pre-check workflows but does not determine eligibility. Eligibility is a protocol-defined determination made by the investigator team, based on criteria documented by the sponsor and approved by the Institutional Review Board (IRB). The pre-check provides input to that determination; it does not substitute for it.
Operational gains for obesity trial teams
The business case for standardized scan-based capture in obesity and metabolic trials is based on five operational categories.
- Lower site-to-site variability. Scan-based capture produces the same structured output regardless of which site staff member conducts the visit, which makes cross-site case review and monitoring more tractable. The same is true across coordinators within a single site.
- Less coordinator time per visit. The measurement and documentation step, which previously required several minutes of manual work, has been streamlined into a guided scan that completes in approximately 45 seconds of processing and produces a structured record directly. The coordinator’s time can be allocated to clinical assessment, protocol management, and participant interaction.
- Fewer measurement-only visits. Where the protocol permits remote check-ins, some measurement-only visits may be reduced, shifted, or replaced by asynchronous remote captures. The participant does not travel to the site for a single data point, and the site does not absorb a slot that does not require clinical assessment.
- Better participant experience and retention support. Long-term obesity and metabolic studies often struggle with attrition. Reducing unnecessary site visits — particularly for measurement-only timepoints — can lower the friction that contributes to dropout. The retention effect is workflow-mediated, but the change in workflow is what the program controls.
- Stronger audit readiness. Structured, time-stamped records support monitoring, QA, and audit processes more directly than free-text site notes. Reviewers can trace when each measurement was captured, under what validation conditions, and within the study’s defined documentation workflow.
These outcomes are operational rather than clinical. They do not change endpoint definitions, statistical analysis plans, or protocol design. What they change is the cost, friction, and consistency of the measurement workflow that surrounds the protocol.
Better measurement workflows support better trial data quality
Trial data quality is not only a function of the sensor or the scan. It is also a function of workflow consistency, capture conditions, recordkeeping, and monitoring discipline. A protocol-defined measurement method can still produce noisy data if the workflow surrounding it is inconsistent across sites, staff, and time points.
Standardized scan-based capture supports data quality in three ways. It reduces process variation across sites by running the same guided sequence each time. It produces structured outputs that support more consistent longitudinal review. And it creates time-stamped records that make monitoring easier — a reviewer can see when each measurement was captured, by whom, and under what quality checks, as recorded by the guided flow.
How does standardized anthropometric capture improve obesity trial data quality?
Standardized capture reduces process variation across sites and staff, making repeated body-measurement data easier to compare, monitor, and document across trial time points. It does not validate the endpoint itself; that remains a question of protocol and analysis plan.
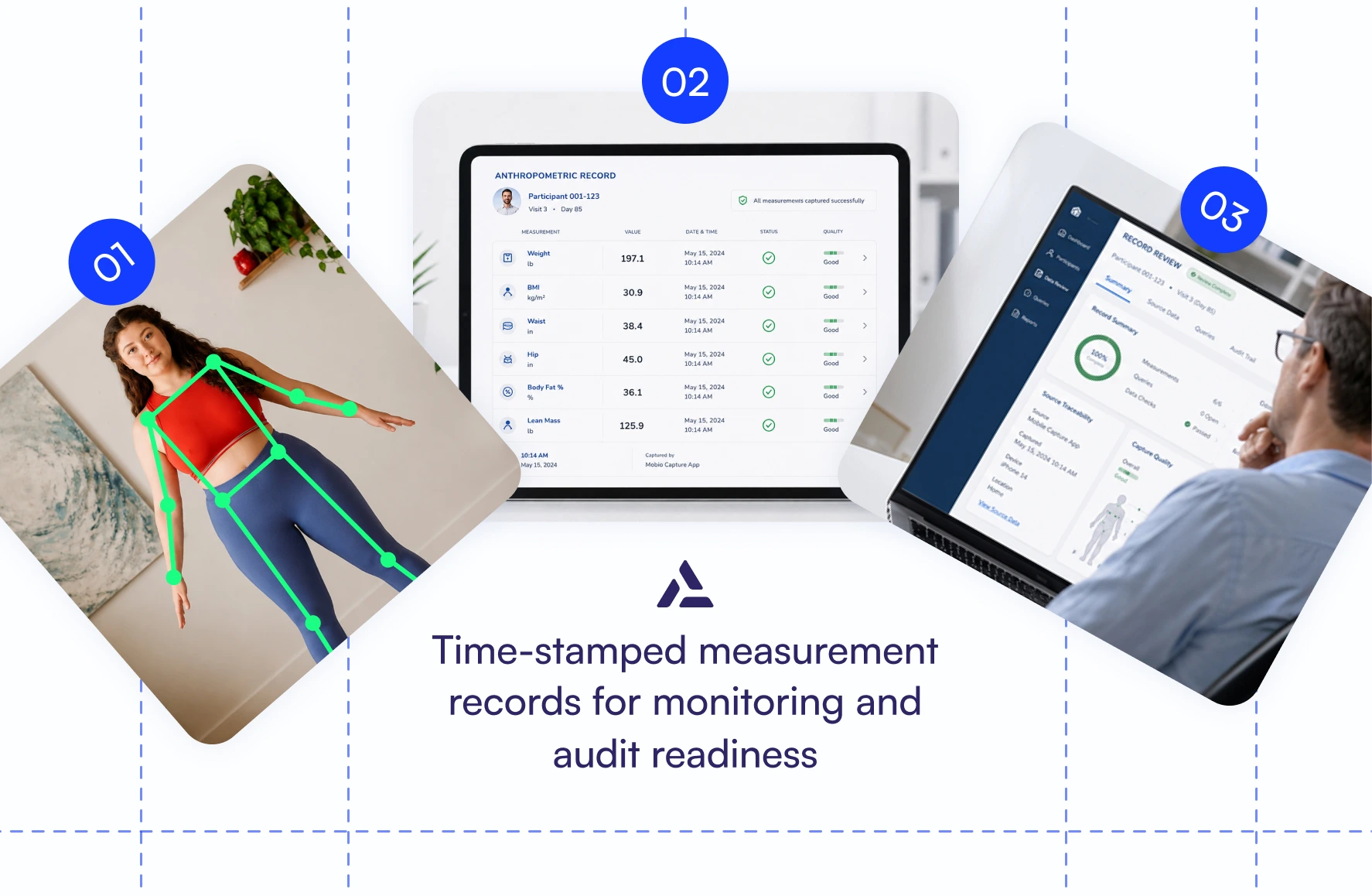
Time-stamped measurement records for monitoring and audit readiness
Sponsors and CROs operate under recordkeeping frameworks that emphasize source data, audit trails, metadata, traceability, and data integrity. The most relevant references are the FDA’s Digital Health Technologies for Remote Data Acquisition in Clinical Investigations guidance (final, December 2023) and the ICH E6(R3) Good Clinical Practice framework (Step 4 final guideline, 2025).
The FDA DHT guidance addresses sponsor responsibilities for DHT selection, verification, and validation of fit-for-purpose use; the use of DHTs to collect data for trial endpoints; risk management; and data retention. FitXpress is positioned to support sponsor workflows within that framework — the regulatory classification for any specific deployment depends on intended use, protocol design, and the sponsor’s risk assessment.
ICH E6(R3) explicitly addresses essential records, source data, audit trails, metadata, data integrity, and traceability. Structured, time-stamped measurement capture supports the documentation and traceability expectations described by the framework — but compliance is a programmatic outcome achieved by the sponsor and CRO through process design, not a vendor deliverable. FitXpress contributes to the recordkeeping posture; it does not replace the sponsor’s responsibility for protocol design, data integrity policy, or monitoring plan.
For trial operations teams, the practical effect is that structured measurement records replace scattered manual notes, inconsistent spreadsheets, and undocumented capture practices. The reviewer can trace when each measurement was captured, the capture quality checks recorded by the guided flow, and the documentation context defined for the study. That trace supports monitoring efficiency and audit readiness — without claiming that the trace alone makes the study compliant.
Clinical and regulatory scope
FitXpress and the mobile body-scanning workflow described in this article support structured anthropometric measurement capture, time-stamped documentation, and remote check-in workflows, as permitted by the trial protocol. They do not replace protocol-defined reference measurement methods (such as DEXA or circumference measurements performed by trained anthropometrists), independently validate clinical endpoints, determine participant eligibility beyond protocol-specific criteria, or guarantee regulatory compliance. FitXpress is positioned as an operational standardization and documentation tool for clinical trial workflows; protocol design, endpoint validation, Good Clinical Practice (GCP) compliance, and sponsor/CRO regulatory obligations remain with the sponsor, CRO, and investigator teams responsible for the study.
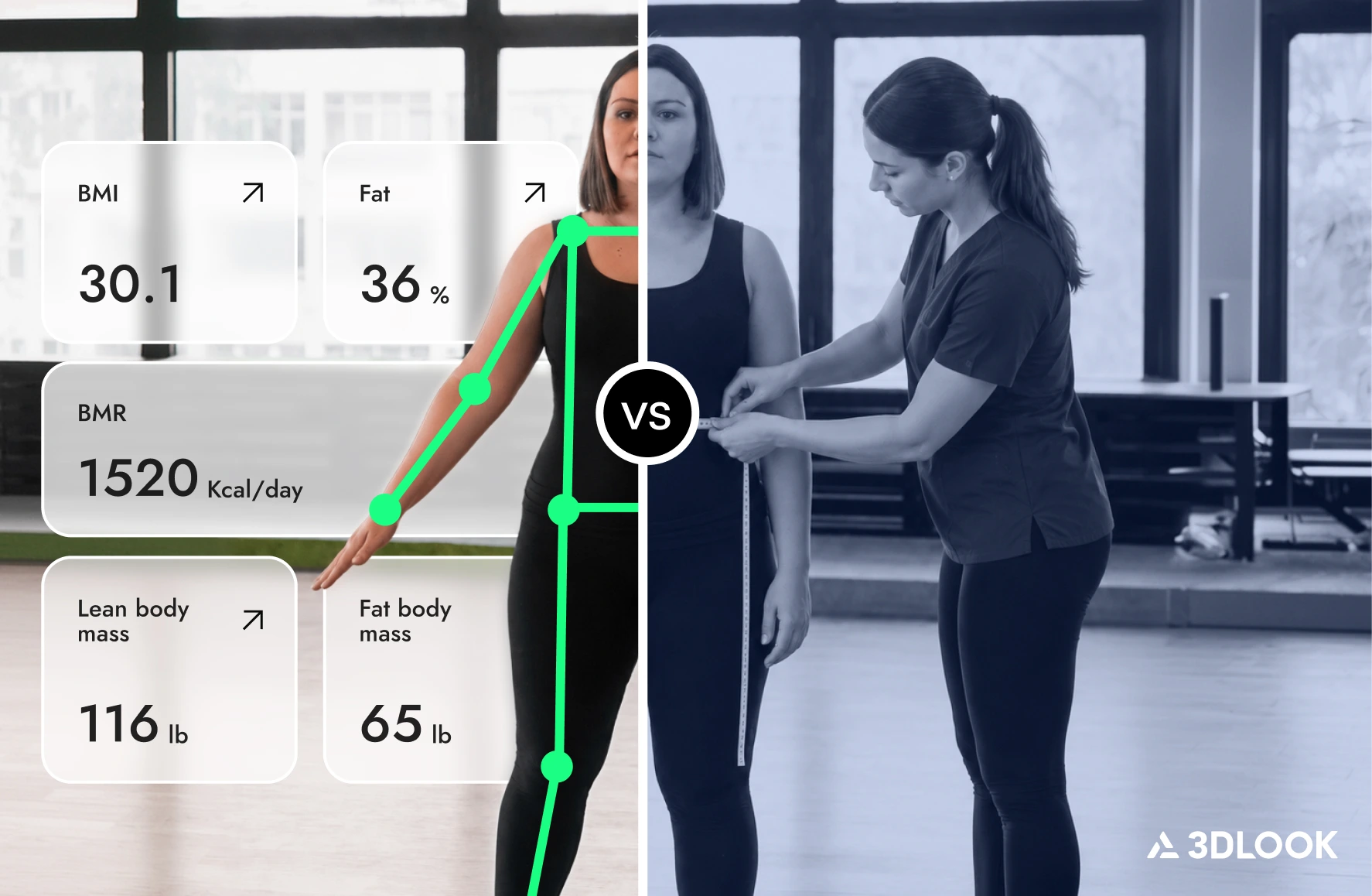
Scan-based capture vs manual anthropometric measurement
The most direct comparison in a clinical trial context is between FitXpress and the manual measurement workflow it replaces. Protocol-defined reference methods serve distinct roles in protocol design and remain in place where the protocol requires them.
| Workflow area | Manual measurement | FitXpress scan-based capture |
| Site consistency | Depends on staff technique and local execution | Standardized guided capture workflow |
| Coordinator workload | Manual measuring and documentation | Scan-based capture with structured outputs |
| Remote use | Limited or difficult to standardize | Supports remote check-ins where protocol allows |
| Documentation | May rely on manual notes or site-specific records | Time-stamped digital measurement records |
| Monitoring | Harder to compare process consistency | Easier to review structured capture records |
| Participant burden | May require measurement-only site visits | Can reduce unnecessary visits in hybrid workflows |
For protocol-design comparisons between scan-based capture and other body-measurement modalities (DEXA, hardware scanners, smart scales), see the related article about AI body scanners vs DEXA scans. The framing there is “different methods, different roles,” which carries through here: protocol-defined reference methods remain where the protocol requires them, and FitXpress supports the standardized capture workflow around them.
Where FitXpress can support obesity and metabolic trial operations
Four operational scenarios cover the most common deployment patterns that sponsors and CROs inquire about.
Multi-site obesity drug trial. A sponsor running a multi-site obesity drug study needs more consistent anthropometric capture across dozens of sites and staff members. FitXpress offers a single guided capture workflow that runs consistently across sites, reducing cross-site variability and facilitating cleaner longitudinal comparisons.
Hybrid GLP-1 study. A CRO running a hybrid GLP-1 study wants to reduce measurement-only site visits while maintaining structured body-measurement records between site visits. FitXpress supports remote check-ins where the protocol allows, capturing scans on the participant’s own smartphone and feeding structured records into the trial documentation workflow.
Academic metabolic health study. An academic research network conducting a multi-site metabolic health study requires a repeatable body-measurement workflow that can be applied consistently across various locations, sites, and participant groups. FitXpress provides the same scan-based capture across the network, with structured records that support cross-network comparison.
DCT platform integration. A decentralized clinical trial platform can incorporate structured capture of body measurements into remote participant workflows. FitXpress supports API/SDK integration with existing platforms, providing the body-data layer alongside the platform’s existing eCOA, eConsent, and remote-monitoring modules.
In each case, FitXpress sits inside the program’s existing protocol design — it does not change the protocol. The change is operational: how the measurement step is executed and how the resulting data is integrated into the trial’s documentation and monitoring workflows.
Built for sponsors, CROs, research networks, and DCT platforms
Five buyer profiles deploy FitXpress in clinical trial contexts, each with a distinct operational priority.
Pharma sponsors running obesity, GLP-1, cardiometabolic, and weight-loss trials use FitXpress to standardize anthropometric data capture across multi-site studies and reduce operational variability in manual measurement workflows.
CROs managing multi-site or hybrid trial operations utilize FitXpress to deliver a repeatable measurement workflow across sponsor programs and clinic partners, thereby reducing the coordinators’ burden and ensuring consistent cross-site documentation.
Academic research networks studying metabolic health and obesity outcomes use FitXpress to establish a standardized scan-based capture protocol across distributed network sites, facilitating comparable longitudinal data collection.
DCT and remote-trial platforms integrate structured body-measurement capture into their existing remote participant workflows via API/SDK, extending their data-capture portfolio without directly operating the scan technology.
Clinical operations teams responsible for site workflows, documentation, and monitoring use FitXpress to reduce the documentation and measurement burden associated with clinical assessment visits, thereby freeing site staff time for clinical and protocol work.
In each case, FitXpress operates within the trial as a workflow-standardization layer. The clinical assessment, protocol design, endpoint definition, and regulatory compliance posture remain with the sponsor, CRO, and investigator team.
Why clinical trial teams need more than “good enough” body scanning
Generic AI body-measurement tools and consumer-grade scanning features can produce measurement estimates that look acceptable in a fitness or wellness context. They do not by themselves deliver what a clinical trial operations team needs.
A trial deployment requires standardization across users and time points, controlled capture conditions, structured outputs that can be queried and compared, traceable records that survive monitoring and audit review, role-based access for sponsors, CROs, and site staff, and a compliance posture that holds throughout the procurement process. Those are workflow and operational properties — not raw measurement properties.
FitXpress is designed for that operational layer. The product is a structured measurement-capture workflow built around the guided scan, with output formats, documentation properties, and integration paths that align with clinical trial workflows. The defensibility of FitXpress in this vertical sits in that operational layer — not in the scan capability alone, which is necessary but not sufficient for clinical trial deployment.
How FitXpress can be deployed in clinical trial workflows
The deployment pattern is the same across the four scenarios above. Five steps connect the protocol design to the capture workflow.
- Step 1 — Define the protocol-specific measurement workflow. The sponsor, CRO, and investigator team specify which measurements are captured at which time points, whether at sites or remotely, and which validation conditions apply. FitXpress configuration aligns with that definition.
- Step 2 — Configure capture steps for site-based and remote use cases. The scan workflow is configured for the relevant capture contexts — coordinator-led on-site, participant-led at home where protocol allows, or both — and tied to the documentation requirements specified by the protocol.
- Step 3 — Train site staff or participants on guided capture. Site staff training covers the coordinator-led capture flow and the documentation handoff. Participant training (where remote capture is enabled) covers the guided self-capture workflow and the support channel for technical issues.
- Step 4 — Use structured records for monitoring and review. Captured records feed into the trial’s monitoring workflow, with time-stamped data available to support sponsor and CRO review and audit response. The use of records in source data review, source data verification, or audit processes is determined by the trial’s documentation workflow.
- Step 5 — Integrate outputs into existing operational or data workflows. FitXpress can support integration with the sponsor’s Electronic Data Capture (EDC), the CRO’s monitoring stack, the DCT platform’s participant workflow, or other downstream systems via API/SDK paths. Specific integration paths are confirmed during procurement based on the trial’s technology stack.
FitXpress is integrated at the measurement step within the protocol’s existing workflow, and the structured output flows into the existing trial data infrastructure. No specialized clinic-facing hardware is required.
Conclusion
Obesity and metabolic trials run on repeated anthropometric measurements, and the operational pressure around that workflow has compounded over time. Multi-site studies, hybrid trial designs, and decentralized check-ins all increase the pressure on measurement standardization. Manual workflows can absorb that pressure up to a point — but they introduce site-to-site variability, coordinator burden, and measurement-only visit friction that scale with the study size.
Scan-based capture is one operational answer to that pressure. It does not change endpoint definitions, protocol design, or regulatory obligations. What it changes is the consistency, friction, and documentation posture of the measurement step that surrounds the protocol.
Next steps
See how FitXpress can support standardized anthropometric measurement capture in your obesity, GLP-1, metabolic, or DCT clinical trial program. Discuss clinical trial workflows with us or book a FitXpress demo to explore the technology in practice with our team.
FAQ
Sponsors can standardize anthropometric measurements by using guided digital capture workflows, consistent measurement protocols, structured outputs, and time-stamped records, thereby reducing variation across sites and staff. The protocol still defines which measurements get captured, when, and against which criteria — the standardization sits in how the capture is executed.
Yes, body measurements can be captured remotely when the trial protocol allows it and the workflow includes appropriate participant guidance, structured capture, and documentation for review. Whether remote capture is appropriate for a specific protocol depends on the timepoint, the measurement, and the sponsor’s protocol design.
CROs can reduce site burden by replacing repetitive manual measurement steps with scan-based capture and by shifting appropriate measurement-only check-ins to remote workflows where the protocol allows. The site continues to handle clinical assessment, protocol-specific procedures, and investigational product dispensing.
Audit trails and time-stamped records help clinical teams review when and how measurement data was captured, supporting monitoring, QA, and audit readiness. They do not, on their own, make a study compliant; compliance is a programmatic outcome the sponsor and CRO achieve through process design.
No. FitXpress is not positioned as a universal replacement for protocol-defined reference methods such as DEXA, certified manual anthropometry, or other validated measurement protocols. Its strongest role is standardized scan-based capture of body measurements, BMI, and body composition estimates for operational consistency, remote check-ins, and documentation support — alongside the protocol’s defined reference measurement where required.
Anthropometric measurements such as BMI, waist circumference, hip circumference, and body composition indicators help trial teams monitor physical changes over time and support study-specific outcomes. The specific set of measurements and timepoints used depends on the protocol and the study’s endpoint design.